THE geniuses behind Medical Student Newspaper have produced some essential reading for all final year medics in the UK, in conjunction with doctors.net.uk. Quack contains all the knowledge one needs to apply for a Foundation post and more. Join the Facebook group.
My contributions included updated versions of stethoscope psychology, depraved revision, a breakdown of the MTAS saga and the WISE words below.
By the way, Medical Student Newspaper has won yet another award nomination. It is in the running for the Best Student Newspaper in the country at this year's Guardian Student Media Awards. Every year since the paper's inception has brought some silverware; fingers crossed.
How to be the coolest, most pimped-out, badass FY1 at your hospital
What you need to know as a first year doc and what you haven’t been told
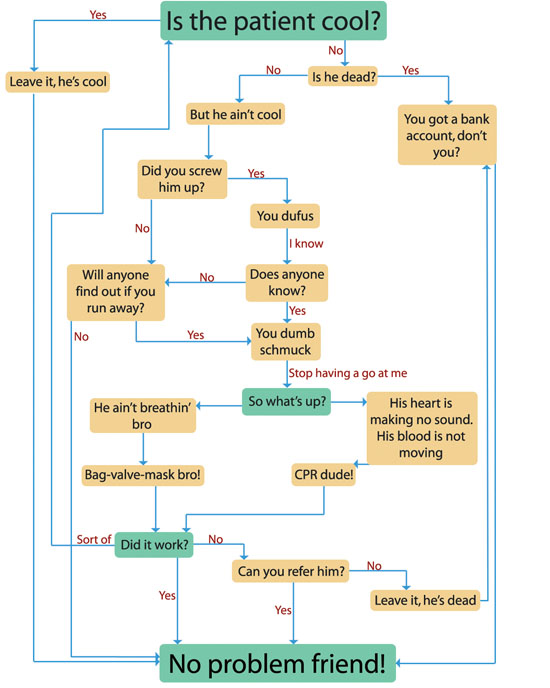
The most up-to-date Advanced Life Support (ALS) algorithm. Use this at any stage during your Foundation Years; acutely unwell patients will be a common encounter and you should feel confident in determining whether a patient is cool or whether they need your help. If unsure, feel free to ask “are you cool?” Don’t be afraid to tell your patients to BE COOL.
There is no one way to be a good FY1, or house officer, as you will still find yourself referred to. However there are certain hints and tips that can be imparted by those that made it through. Intact. Unscathed. Ready to fight another day. ONWARD!
First and foremost, your first year as a doctor should be about enjoying yourself. Never forget this. There are many similarities to life at medical school; you will probably live in halls, go out too much and make lots of new friends. The only real differences are that you can’t bunk off anymore, but you do get paid.
The single greatest fear of a new doctor is that they will do some harm to a patient. This, whilst not impossible, is improbable. The reason being that you have spent four to six years learning how to do the opposite.
You are so imbued with misplaced self-doubt when you start working that you end up being over cautious. This is normal. Don’t worry about making mistakes, just concentrate on enjoying yourself and the rest will flow.
Perhaps the one gem of information I wish I had been given before I started was that you did not need to be top of the class at medical school to succeed in your first year of work.
In fact, where you ranked has no correlation whatsoever to how you will perform and you should put it out of your mind entirely.
If the comparison of FY1 to medical school can be extended, then the first week is Freshers’. With most junior medical staff now starting at the beginning of August every year, the hospital will be atwitter with introductions and nice-to-meet-yous when you start.
The first few days are rarely taxing. They normally consist of induction talks, orientation sessions and a gradual easing into the job.
You might turn out to be one of the unlucky punters that kicks off work with an on-call. Daunting it may be, but on-calls are fantastic learning opportunities. Asking for help is something you should never be afraid of doing in your first year. People will fully expect you to ask the most inane of questions, even if you feel like an idiot. Get over that embarrassment and ask – better that than goofing up something easy.
There is also no shortage of people to ask. Obviously your immediate seniors are a logical first step, but the resource you will invariably draw upon throughout your junior years is the nursing staff. If you take one piece of advice away from this article, make it this: be nice to nurses.
Nurses can make your life so much easier if you acknowledge their existence and value their contribution, and they can equally give you grief if you piss them off.
Nurses, like anyone else, don’t like being talked down to by snooty doctors. If you’re not sure what fluids to write up, or what the dose of metoclopramide is, asking a nurse is a good first move.
Having said that, nurses go through a learning process too and might be just as green as you. If you’re unsure about any advice given, there’s no harm getting a second opinion. You will find that the ability to know what is duff advice and what is good sense develops quickly and naturally.
A further word about those nurses. Most FY1s will be ward-based and whilst it is useful to be nice to nurses on-call, it is imperative to establish good relationships with the nurses on your own ward. They can be inordinately helpful if you’re mates. Not to mention that if you can have a laugh with the nurses, social workers, ward clerks, physios, OTs, HCAs or medical support workers on your ward, your job will all the more fun.
This provides a convenient segue onto what is likely to be the bane of your life during the Foundation Programme. Assessments. You thought tick-boxes and form-filling ended with graduation. I laugh at your foolishness.
Working well with those around you will stand you in very good stead for a key part of your overall assessment, the min-ePAT. Out of all the nonsense you are forced to complete in your first year, this is a very useful exercise.
On two occasions you are required to nominate twelve co-workers, of whom only a limited amount can be doctors, to anonymously say what they think about you. As you can imagine, the ability to be frank allows your colleagues to give you what can frequently turn out to be valuable advice.
All that need be said about the rest of your assessments is that the sooner you get them out of the way, the better. Try not to leave yourself a week to get all the forms filled in, it is no fun.
To reiterate, it is imperative you concentrate on having fun in your first year. It comes only once and just about every doctor you meet looks back on their house officer year with great nostalgia and fondness. No amount of hints and tips from seniors will replace your learning-by-doing, so try not to be wallflower.
If something that interests you is happening, be it inserting a central line or an appendicectomy, try to get involved. Be in the right place at the right time, but don’t be a dick – share out opportunities with friends.
Developing confidence comes far more easily to some than others, but ultimately the only occasion it matters is when a patient’s health is in question. If you are seeing someone in A&E or on the ward and you are unhappy about something, never worry about ‘bothering’ your seniors. Whilst it may be surprising to some, no one will criticise a new doctor for being too safe.
Lastly, if you are one of those keen young things that wants his or her name in lights, your first step would be to leave medicine. However if you want to stay, you might want to consider getting involved with an audit, a presentation or two (most hospitals expect a Grand Round presentation from all the juniors) and if you’re extra ambitious, a publication.
Having said all that, none of these are necessities. The only compulsory objectives for an FY1 are consolidating your medical knowledge (it’s up there somewhere, even if it doesn’t feel like it), seeing patients, getting organised, using your hands, extra-curricular high jinx and wild japes. These are integral to being a good doctor. Good luck and get ready to work like a HO.
Originally published in Quack: Foundation School Guide.
Diagram inspired by ALS guidelines and a flowchart from Antarctica, by Kim Stanley Robinson.
Labels: junior doctors, medicine
My regular column in Medical Student Newspaper has been reprised this academic year. This year it is, of course, 'F2. Woohoo.' Originally published in the October issue,
I’M CANCEROUS. Yes that’s right, I’m back for a fourth year running. This year, I come to you from the dizzy heights of the most superlative foundation doctor there is, THE MIGHTY F2.
A new generation of fresh-faced F1s replaced me and all my ilk. Now I’m supposed to know shit, you know, and stuff.
A&E’s a funny place to work. Over 90% of you will spend four months ‘on the medical front line’ as I am now. Unless you choose to pursue this field (ya crazy fool), your A&E rotation will be the job that brings you more excitement, boredom and frustration than any other. Mostly frustration.
No longer is the emphasis based on diagnosis, which is what draws so many into medicine, but on exclusion. Can you send this healthy 30 year-old chap home...are you SURE he hasn’t had an MI? Let’s refer him to the medics for a twelve-hour trop and take up a hospital bed just in case. It’s mind-numbingly un-stimulating at times.
There are many positives about working in A&E. Exposure to a wide range of problems, dealing with genuine emergencies, seeing instant results. My particular hospital has four great consultants and as St. George’s is a Centre of Excellence for countless specialties, I see some crazee sheeyrt.
However the one overwhelming negative is that it is A&E. There is no area of medicine that has been toyed with by the government as much as the emergency department.
Because waiting times are so easy to quantify and brag about before an election, A&E is a convenient place to pull numbers from. It is also one of two first points of contact for patients. The other is, of course, general practice, which has been tinkered with almost as much, chiefly to the detriment of A&E departments.

The ridiculous lack of sufficient out-of-hours GP provision, NHS dentists, the creation of stop-gaps like NHS Direct and obscene waits for GP appointments mean we are inundated with complaints that are neither accidents nor emergencies.
Yet each person that attends A&E has to be seen, diagnosed, treated and moved out of the department in four hours.
As all five Rohinplasty readers will know (it’s going up), I am obsessed with a solid evidence base. I use that as a chat up line sometimes. Anyway, one would like to think that those responsible for these four hours used all the available data to construct a sophisticated model of a working A&E and thus extrapolated a suitable figure.
The truth is probably more along the lines of pin-the-tail-on-the-number, with an arbitrary figure being plucked from the air.
The reality is a shambles. Of course no standard duration can be applied to A&E patients, as there is no one type of A&E patient. Some are out within ten minutes but some need several hours.

A far more sensible system, as I’m sure an honest government would concede, would consist of clinicians deciding how long each patient needed to be safely dealt with.
However politicians make decisions, not doctors, so that ‘four hour waits’ can be political weapons.
Only 2% of patients are allowed to ‘breach’.
I figured, like many others, a cavalier attitude was the way forward and thought I would ignore breaches and put the patient first. The NHS doesn’t work that way.
Unwell patients often need to stay in A&E until they are stable enough to be transferred. Pissheads need to sober up before they go.
The Medical Assessment Unit, or MAU, that most of you will be familiar with by now, owes its existence to the four-hour-wait. MAUs were created to stop the clock. The vast majority of patients admitted to a hospital come under the care of the general physicians. Hence all medical patients now go to MAUs where there is no timer.
There is no guarantee they will be adequately treated by the time they arrive there and there is no guarantee they will be seen by the doctors looking after them, hence negating the entire reason for the four hour rule.
I must be careful with what I say about my employer, so suffice it to say that unfortunately cooking the books MAY OR MAY NOT OCCUR at SOME hospitals around the country. Will that sound sufficiently vague in court?
Picture the scene. A patient needs a urine dipstick to make a diagnosis of a UTI. However a nurse is off sick and the nursing staff is over-stretched. No one gets the urine sample. The patient breaches. If this breach were recorded perhaps management would see that missing nurse’s value.
However if the number of breaches is the same as on any other night, the hospital realises she’s unnecessary and sacks her. They congratulate each other on more money saved. The system is broken, nothing changes.

We have some bizarre A&E mentality now that stipulates the customer is always right. But the patient is rarely first.
Nurses will drive you slowly mad with a phrase you will quickly grow tired of, “come on, your patient’s about to breach.” I normally cave.
Title reference to Nine Hours to Rama.
Labels: A+E, medicine, NHS, Rohinplasty articles


Diversity Writer of the Year

Runner-up Columnist of the Year
Nominated Features Writer of the Year





It's the Pirates
Yam Boy
Video Wallah
Shiva Soundsystem
Within / Without
Saheli Datta
Random Acts of Reality
NHS Blog Doc
The Oracle

Turbanhead
HERStory
Ethno Techno

2. Rohinplasty (series)
3. Medical student teaching (series)
4. What your stetho says about you
5. Revision: IT BRINGS DEATH
6. Things you kids won't see (series)
7. Tsunami Politics
8. Churchill: Let the fakir die
9. If it looks like a quack...
10. Ten million missing girls


Real Doctor
They hate you
Incendiary views
Scrooge McDoc
Suspicious behaviour
The Renal Angle
The bastard son of MTAS
All Hallow's A&E
Quack



August 2005
September 2005
October 2005
November 2005
December 2005
January 2006
February 2006
March 2006
April 2006
May 2006
June 2006
November 2006
December 2006
February 2007
May 2007
June 2007
July 2007
August 2007
October 2007
November 2007
February 2008
March 2008
April 2008
May 2008
July 2008
December 2008
-->